
Ebola’s ability to travel has been well publicized, but there is another story: one of immobility. In West Africa, research materials that contribute to improving knowledge about the disease such as blood samples and patient records have been trapped or entangled in the “hot zone.” In some circumstances, the virulence of such materials appears to pose a risk to biosecurity that may be greater than their ability to help mitigate that risk. In times of uncertainty, fear may trump established policies about how to manage the flow of people, information, and research materials. For instance, while the World Health Organization (WHO) has been opposed to travel restrictions to ensure continued circulation of health workers, the home institutions that employ such workers may choose to impose such restrictions. In such cases, prevention is seen as a preferable alternative to quarantine should health workers return with infection. Yet, physicians and health workers who have been able to travel between makeshift treatment camps in Africa and the resource-rich laboratories and medical centers in the Global North have been frustrated to realize that perceptions of the intensity of the hot zone functions to freeze the otherwise relatively fluid channels of global biomedical infrastructure.

Airmen from the Kentucky Air National Guard’s 123rd Contingency Response Group, as they were carrying whole blood to a waiting U.S. Air Force C-130 Hercules at Léopold Sédar Senghor International Airport in Dakar, Senegal. The blood was being sent to Liberia to support U.S. troops deployed for Operation United Assistance, the U.S. Agency for International Development-led, whole-of-government effort to respond to the Ebola outbreak in West Africa.
Since the time of Pasteur in the late nineteenth century, blood, tissue, urine, and stool samples collected at the sites of epidemics have been crucial resources for increasing knowledge about infectious disease (Anderson 2010; Neill 2012). With the rise of cryopreservation in the decades after World War II, blood samples could be accumulated and shipped to biomedical laboratories for analysis (Radin 2014). Often these samples would travel in coolers or liquid nitrogen Dewar flasks held on the laps of researchers as they flew back from the field. Today, the biospecimen—both cryopreserved as well as freshly collected—continues to be an invaluable resource for learning about emerging infections diseases. Yet, the perceived virulence of Ebola, the great uncertainty about its mechanisms, and the resource challenges that undermine efforts to adhere to best practices has made it extremely difficult to traffic in blood. It has made it hard to move biospecimens at all, despite the existence of special protocols for doing so (WHO 2014).
In November of 2014, for instance, Frederique Jacquerioz, a physician and researcher based at Tulane University Medical School, presented a dispatch at the American Society of Tropical Medicine and Hygiene (ASTMH) annual meeting in New Orleans titled “From the Hot Zone: A Clinician’s Perspective on Confronting Ebola Virus in West Africa.” She had been in Liberia several months earlier and described the challenges to treatment and knowledge production presented by the logic of containment.
These challenges begin with the protective gear that is considered be most effective in reducing transmission of Ebola virus from patient to health care provider. Ease of movement in personal protective equipment (PPE) is an acquired skill. It is not something that can be learned in 20 minutes. PPE also hampers existing skills. One cannot listen to lungs or put in an IV easily while wearing the so-called “moon suits.” In the tropical climates of Western Africa, a health worker can only perform a short stint in such gear before taking a break to hydrate.
In such circumstances, the medical chart becomes an important means of sharing information between health workers who are rapidly cycling on and off shifts. Jacquerioz explained that keeping track of fluid loss, which is so extreme in Ebola patients that it often comes to be measured by buckets, is an essential component of care. However, since paper medical charts often are splattered with droplets of bodily substance in the course of care, they can quickly become classified as a biohazard. This means that it is not easy for medical records to travel beyond the clinic.
Patient information has been making it out of the hot zone through health care workers’ use of the cameras on their smartphones. Taking pictures of the records is emerging as a makeshift workaround, but may not lead to data aggregation for analysis. The idea that “big data” could be used to combat Ebola is undermined by the fact that there is not enough data; the data that matter are still hard to get (Wall 2014). Most of the big data claims are based on reports of suspected or actual cases by those who hear about or observe symptoms of infection. They have not been based on the kind of validated patient and genomic information we might assume is at the heart of medical big data, in part because obtaining that data is incredibly difficult both technically and bureaucratically.
Richard Preston, author of the 1990s technothriller The Hot Zone, recently wrote in the New Yorker about how hard it has been to circulate Ebola blood samples (Preston 2014). While some blood made it out of Sierra Leone in May, “[a] thousand more vials of human blood with Ebola in them are sitting in freezers in Kenema waiting for bureaucratic clearance so that they can be flown to Harvard and sequenced in the machines, and scientists can see what the swarm has been doing more recently” (Preston 2014).
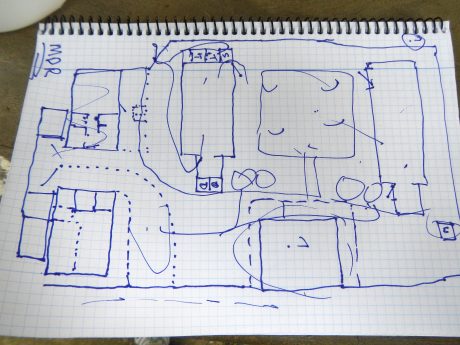
A rough sketch by a Doctors Without Borders, i.e., Médecins Sans Frontières (MSF) logistician depicting plans for the construction of a “hot zone” to be located in Lagos, Nigeria.
Other high-tech interventions have shown their limits in West African contexts. The point of care test device known as POC-T, developed for use in the emergency rooms of Euro-American hospitals, has been adopted as a way of quickly obtaining vital statistics in the hot zone. But because it is hot in terms of temperature as well as virulence, these devices frequently overheat and fail. Jacquerioz reported that she and her peers had to take time to use ice that was already in short supply to cool the devices so function could be restored.
It is not only research materials and data that have been frozen in place. In the Q & A session following Jacquerioz’s presentation at ASTMH, a researcher and physician who identified himself as having “named the bloody thing” in the 1970s raised the question of nursing care. He asked whether or not those who had seroconverted and survived Ebola were being enrolled as frontline support in caring for patients in the hot zone. The answer is yes. Jacquerioz emphasized that right now, “the real heroes [of the West African epidemic] are the people who cannot or do not leave.”
Beyond those international health care workers who choose to remain in the hot zone, a recent article in Wired magazine highlights the complex social role of individuals whose agency is more mediated; those who have survived and stayed to perform caring labor. “All their possessions are gone, destroyed while they were sick to avoid contamination. They feel shunned, even as they work to save others” (Hayden 2014). Recovery in such a situation has become situated as a biological and social imperative to remain at the epicenter of suffering. The international public health community may view nurses in places such as Sierra Leone as heroes, but their return to the hot zone is also a result of the stigma they experience by having been ill. Inadequacies in health infrastructure and fear about the spread of infection that make it difficult for biospecimens and patient information to circulate also contribute to the circumstances that make it difficult for survivors to move on.
Even those who can leave the hot zone have found that the stigma of having been exposed to Ebola constrains their ability to participate in efforts to share knowledge about the epidemic. At the ASTMH—among the most important gatherings in the field of infectious disease—the Louisiana Department of Health and Hospitals attempted to impose quarantine restrictions on researchers traveling to the meeting from any of three Ebola-affected countries (Governor’s Office of Homeland Security and Disaster Preparedness 2014).Prospective meeting participants were greeted with the threat of isolation:
Welcome to New Orleans
- Within the past 21 days, have you traveled from Liberia, Sierra Leone, or Guinea?
- Do you have flu-like symptoms and a fever?
- Have you been exposed to someone who was suspected or known to have Ebola?
If you answered YES to questions 1 or 3, please call our 24-Hour hotline…
As the epidemic continues to unfold and public health officials continue to make decisions based on partial information and with inadequate resources, people (survivors) and things (medical charts, blood samples) are being both produced and contained by the hot zone. Getting anything or anyone out of the hot zone, even a recovered patient or healthy researcher, has become a chilling dimension of this epidemic.